
The situation overview is produced by Nutrition Development Partners with support from UNICEF INDIA and Global Nutrition Cluster Technical Alliance. It serves to document and monitor the situation and needs of vulnerable women and children along with provision of information on effective nutrition sector response amidst the COVID-19 pandemic.

Anganwadi worker Vidhya Jain (middle) talking to pregnant women and young mothers about the importance of nutritious food at Jethana B Anganwadi center, Rajasthan, 24 Dec 2020. Photo © Sri Kolari
Content
1. Introduction
2. Executive Summary
3. Background
4. Nutrition Conditions
4.1 Preschool aged children
4.2 Women
5. Status of Essential Nutrition Services
5.1 Preschool children
5.2 School children
5.3 Adolescents
5.4 Women of reproductive age
5.5 Nutrition social behaviour change communication activities
5.6 Food fortification
6. Nutrition Sensitive Sector Updates
6.1 Food Security
6.2 Health
6.3 ECD
6.4 WASH
6.5 Livelihoods
6.6 Governance
6.7 Gender and Equity
7. Key Global Updates
8. Case story highlighting COVID-19 specific innovations/initiatives
9. Abbreviations
———–
1. Introduction
This situation overview is produced by Nutrition Development Partners with support from UNICEF INDIA and Global Nutrition Cluster Technical Alliance. It serves to document and monitor the situation and needs of vulnerable women and children along with provision of information on an effective nutrition sector response amidst the COVID-19 pandemic. It also attempts to draw attention to what critical and granular data is missing to comprehend the impact of COVID-19 on nutrition in India.
The quarterly report is prepared by collecting relevant information from concerned partners and gathering the related and available data from government monitoring system and key assessments. It is then shared with all nutrition partners and is also archived at https://poshancovid19.in/. The report present most recent available information up to end of September 2021. Considering the rapidly changing COVID situation, best possible efforts are made to be specific on the time frame where data precedes the specific reporting period of July-September 2021.
While experts continue to monitor if India will experience a third COVID wave, there is a real chance that the broader impact of COVID on families and communities will last longer, possibly even for years. It is the intention of development partners to continue these efforts to document the impact of COVID on nutrition with updates on a quarterly basis.
For any corrections and/or comments, please contact <poshan@unicef.org>

Latha Raju Masaur breastfeeding her newborn son (DOB: 03 December 2020), Jethana village, Rajasthan. Photo © Sri Kolari
2. Executive Summary
This situation overview is produced by Nutrition Development Partners with support from UNICEF INDIA and Global Nutrition Cluster Technical Alliance. It serves to document and monitor the situation and needs of vulnerable women and children along with provision of information on an effective nutrition sector response amidst the COVID-19 pandemic.
India has a great population but also was greatly affected by COVID-19 as noted from the numbers of COVID-19 cases and deaths. In terms of nutrition, the most recent data on nutritional status (NFHS5) were collected prior to the COVID-19 crisis and showed that progress in the reductions of malnutrition has slowed down on many indicators in early 2020. It is not unlikely that malnutrition has increased during the pandemic, more so amongst the vulnerable groups in underprivileged communities. As of now, there are no available data on the nutritional status of children and women after the onset of the COVID-19 pandemic and lockdown (starting in April 2020). The impact of COVID-19 on Infant and Young Child Feeding practices has not been documented. Evidence is emerging on the negative impact of the pandemic on women’s diets with greater effect among women from marginalized groups.
Tracking reports from 14 states show that by September of 2021 child growth monitoring has been restored conducted through home visits or at the Anganwadi centres. The take-home rations for children and pregnant and lactating women under Integrated Child Development Services scheme as well as Nutrition Rehabilitation Centers are reported largely operational in all States/UTs. Some studies and surveys have documented instances of take-home rations not received by the intended beneficiaries and sharing among the household members. There have also been reports of disruption in the delivery of essential nutrition services by frontline workers when additional responsibilities of COVID-19 tracking and prevention counselling were added. By the third quarter of 2021, schools have begun to reopen but Mid-day Meal scheme used alternative delivery mechanisms to ensure service delivery in 35 of 36 States/UTs through food transfers or food security allowance. There have also been reports of some of the Mid-day Meal beneficiaries either not receiving benefits or receiving less than their entitlements.
The available HMIS reports until May/June 2021 show reductions compared to pre-Covid reports in terms of essential nutrition services such as Vitamin A supplementation among preschool children, IFA supplementation and deworming among children aged 5-9 years, school children attending 6-12 class and out of school adolescent girls 10-19 years at Anganwadi Centers. Also reported was a reduction in pregnant women receiving four or more antenatal care check-ups and institutional deliveries as compared to the pre-COVID period.
The PMMVY maternity benefits programme is reported largely operational. Nutrition social behaviour change communication activities are being conducted and special campaigns such as World Breastfeeding Week and Poshan Maah are being celebrated. Food fortification initiatives are ongoing in several parts of the country.
Food insecurity remains a question as a number of assessments across the country identified issues since the start of the pandemic. Greater risks are possibly found among the disadvantaged groups, during and after the national lockdown period. Targeted public distribution of food grains is reported to provide much needed relief to vulnerable families across the country. The disruptive impact of COVID-19 pandemic on livelihoods has been documented, especially among women and poor and vulnerable families.
Nutrition development partners recognizing the threats of the COVID-19 pandemic updated the Commitment to Action for Nutrition. In these shared advocacy efforts, the partners committed to 6 key areas for urgent action with strong recommendations for rapid restoration of essential nutrition services, but also to expanded and strengthened service delivery in urban and rural zones of food insecurity and areas with large numbers of impoverished and disenfranchised populations.
3. Background
Due to population size, India has some of the highest numbers of COVID-19 cases and deaths (https://covid19.who.int). As of 8th October 2021, there were almost more than 34 million people in India reported as infected by COVID-19 and 450,000 deaths. The pandemic is still at large as evidenced by more than 2.4 million active cases, more than 20,000 daily new cases and official reports of around more than 270 COVID-19 related daily deaths (https://www.mygov.in/covid-19). There have been a remarkable mobilization of resources to produce actionable data on COVID-19 but also calls for better quality and more granular data which are critical for public health interventions.
The most recent available data on nutritional status were collected prior to the COVID-19 crisis. The NFHS- 5 results for 22 states /UTs show that progress in reductions of malnutrition has slowed in early 2020.
- One third of children under-five are stunted and one out of five are wasted (CNNS 2018)
- High prevalence of wasting found in north and central India from July 2019 to Jan 2020 (NFHS-5)
- Over half of women of reproductive age are anaemic (53.1% – NFHS-4). Anaemia among children from 1 to 4 years – 40.5% (CNNS 2018)
- Only 6.4% of children 6-23 months receiving a minimal adequate diet (continued breastfeeding, appropriate frequency of feeds and dietary diversity) (CNNS 2018)
Early scenarios predicted that COVID and the potential response would affect the poor, vulnerable and marginalized populations more severely than others due to direct effects of infection and indirect effects of reduced access to foods, essential health / nutrition services and potable water/hygiene. Attention was also drawn to the probable diversion of leadership focus and resources for nutrition as attention shifted to COVID-19 mitigation and management.
It is not unlikely that malnutrition has increased during the pandemic, more so amongst the vulnerable groups belonging to underprivileged communities, noted the national president of the Indian Academy of Pediatrics (Indian Pediatrics July 2021). Updated global modeling estimates suggested that by the end of 2022, the world could face an additional 9 million wasted children, 168,000 additional child deaths and 2 million women with anaemia (Nature Food July 2021). As India represents a large proportion of the global population, up to one third of these cases of wasting, anemia and child deaths may occur here.
Following the COVID-19 pandemic crisis and closure of Anganwadi Centers (AWCs) in April 2020, the Government of India ordered Anganwadi workers to deliver the take-home rations to beneficiaries at home. Similarly, the government also advised all States/UTs to provide hot cooked meals or food security allowance comprising of food grains and cooking costs (or its equivalent in pulses, oil) to all children covered under Mid-day Meal (MDM) scheme during the closure of schools.
To address the threats to livelihoods, diets and reduction of services, the Government of India announced a broad reaching relief package including additional rations/pulses through the Targeted Public Distribution System (TPDS), cash transfers to Jan Dhan accounts, increase in MNREGA wages (guaranteed wage labor) along with strengthened social protection schemes and insurance for health workers. These actions along with the Pradhan Mantri Garib Kalyan Yojana provided social safety nets services to millions of households across the country (PMGKY, August 2021). The Prime Minister restated the importance and the commitment of the government to the priority of reduction of malnutrition during Independence Day speech on 15th August 2021.
4. Overview of Nutrition Conditions
4.1. Preschool children (under five years of age)
- Up to September 2021, there are no available data on child nutritional status after the onset of the COVID-19 pandemic. There have been concerns that child malnutrition is likely to have worsened. However, concrete evidence on the impact of COVID-19 on child undernutrition and whether it is compounded by other prevailing threats and seasonal morbidities remain unknown. Routine programme data including regular growth monitoring data from Integrated Child Development Services (ICDS) are also not publicly available. Similarly, the conditions of acute malnutrition among children, a key nutrition indicator during emergencies are also not known. The data on admissions into Community-based Outpatient – Management of Acute Malnutrition (CMAM) programme and inpatient – Nutrition Rehabilitation Centers (NRCs) data are not available on public domain. Hence, there is a data gap on the impact of COVID-19 on acute An urgent call has been made for the nutrition community to renew the focus on nutrition and to generate evidence to address malnutrition in the context of the COVID-19 pandemic (IFPRI – Menon et al. 2021).
- The impact of COVID-19 on Infant and Young Child Feeding (IYCF) practices has also not been broadly documented. Information is limited on exclusive breastfeeding and complementary feeding including dietary diversity and feeding The critical lifesaving intervention of providing breastfeeding to the newborn child in the first hour of life can significantly reduce newborn mortality. Early initiation of breastfeeding as reported by the Health Monitoring Information System (HMIS) has been lower than pre-pandemic levels: reported at 80.6% in October 2019, dropped to 48% in April 2020, recovered to 77% in October 2020 but then there has been a steady decline again at 65% in April 2021 and 51.2% in May 2021.
4.2. School age children and adolescents
- There are no available data yet on the impact of COVID-19 on anthropometric status of populations from 5 to 19 years of age.

Patients waiting at the OTP Ward at the Dungapur District Hospital, Rajasthan 22 Dec 2020. Photo © Sri Kolari
4.3. Women of Reproductive Age
- There are no available data yet on the impact of COVID-19 on women’s nutritional status including indicators such as body mass index, gestational weight gain or pregnancy complications.
- There have been no assessments on the prevalence of anaemia among women after the pandemic. As per the HMIS reports, the prevalence of anaemia (hemoglobin <11 g/dl) among tested pregnant women was 69.8% in March 2020 versus 62.0% in June.
- There have been no assessments on the impact of COVID-19 on birth As per the HMIS reports, Out of total children weighed at birth, the proportions reported to have low birth weight (weighing less than 2.5 kg) during March 2020 versus May 2021 is 11.6% versus 12.1%. These are not considered to be accurate estimates as data are affected by heaping and are not representative of the overall population.
- Evidence from two studies reported a negative impact of the pandemic on women’s diets with greater effect among women from marginalized Decrease in consumption of nutrient rich food groups like meats, eggs, vegetables, and fruits and increased food and nutrition insecurity was reported by women in low income households from 10 states(Dalberg study, May 2021) . Decline in household food expenditures and women’s dietary diversity were found at national, state (UP, Bihar and Odisha and district level through comparisons of May 2020 to May 2019 data. (Tata-Cornell Institute for Agriculture and Nutrition study, July 2021).

Anganwadi worker Leena Bhat playing with the children of the Jethana Aanganwadi Center, Rajasthan, 24 Dec 2020. Photo © Sri Kolari
5. Status of Essential Nutrition Services
The HMIS data provide monthly report on essential nutrition service provisions and are publicly available only up until May 2021. Selected anaemia related indicators are available up to June 2021 under AnemiaMukt Bharat campaign.
UNICEF conducts monthly tracking of continuity of services in the 14 most populous states of the country representing over 85% of the population. These states are Assam, Andhra Pradesh, Bihar, Chhattisgarh, Gujarat, Jharkhand, Karnataka, Madhya Pradesh, Odisha, Rajasthan, Uttar Pradesh and West Bengal. The UNICEF Continuity of Services tracking during September 2021 found that the AWCs are still closed in all States (except Chhattisgarh, Maharashtra, Rajasthan and Telangana.) WFP conducts quarterly tracking of ICDS and MDM schemes at national and sub-national levels. The currently available report from January to April 2021 found that the AWCs remained closed in 25 States/UTs (70%) until April 2021. Both tracking found that though the AWCs remained closed in most States/UTs, the essential ICDS services including supplementary food, immunization and growth monitoring are reported operational in most states.

Reena Patidar (Right) ASHA worker talking to Latha Raju Masaur (Left) about the importance of the breast feeding during regular home visit, Jethana village, Rajasthan, 24 Dec 2020. Photo © Sri Kolar
5.1. Preschool children (under five years of age)
- Vitamin A 1st dose was reported to be received by 56.4% of children during May 2021 which is lower than 65.8% reported during the lockdown period of May 2020 (HMIS.) Mass Vitamin A supplementation was reported to be conducted during August 2021 in Madhya Pradesh, Odisha and Uttar Pradesh. (UNICEF Continuity of Services Tracking, August 2021)
- Deworming tablets were provided to 1.0% children aged 12-59 months during June 2021 which is similar to 1.1% reported during the pre-pandemic report of March 2020 (HMIS.) The data for deworming may present low coverage as the selected data does not correspond to the dates of the biannual National Deworming
- The data on IFA supplementation to children aged 6-59 months for June 2021 also shows slight reduction than what was reported before the pandemic in March 2020: 15.3% vs. 14.1%. (HMIS)
- Bundling of services (IFA supplementation with Vitamin A supplementation or mass screening for acute malnutrition during Vitamin A supplementation) was conducted in Madhya Pradesh, Odisha, Uttar Pradesh and Chhattisgarh. (UNICEF Continuity of Services Tracking, August and September 2021)
- Provision of Take Home Rations (THR) for children aged 6-72 months are operational in all states, except partially available in Jharkhand (UNICEF Continuity of Services Tracking, September 2021.) Door-step delivery of THR is being done monthly or once every two months. The THR basket considerably vary across the States/UTs and the food items include fortified blended foods, eggs, sorghum powder, Chikki (snack food made from nuts and jaggery), milk, and skimmed milk powder (WFP ICDS Tracking, January to April 2021.)
- In Jharkhand and Rajasthan, sharing of the THR for children with other family members was reported during August 2020 increasing the risk of dilution of the intended nutritional benefits (IDinsight May 2021) Nearly 70% under-3 malnourished kids in rural Jharkhand were reported not to the receive additional nutrition support during January to June 2021 (Right To Food Campaign survey). The National Human Rights Commission of India issued notice calling for a detailed report to the Government of Jharkhand and Ministry of Women and Child
- Growth Monitoring and Promotion is active in all 14 States except Gujarat (UNICEF Continuity of Services Tracking, September 2021.) Growth monitoring are operational in 29 States/UTs (80%) and are being conducted through home visits or at the AWCs. (WFP ICDS Tracking, January to April 2021)
- In Rajasthan, the pandemic and lockdown reportedly created disruption in delivery of essential nutrition service by frontline workers. Door step delivery of THR, IFA supplements and growth monitoring through home visits was planned in many states but was deprioritized when additional responsibilities of COVID-19 tracking and prevention counselling were added. (IDinsight 2021)
- In one district in Uttar Pradesh, essential services (VHNDs, health and nutrition counseling, IFA supplements distribution, ANC check-ups, immunizations and growth monitoring) were reported to be reduced substantially during lockdown (up to 98%), except for home visits and THR (∼30%) and utilization of most services did not improve after the lockdown (IFPRI and Alive & Thrive – 2021)
- Provision of Community-based Management of Acute Malnutrition (CMAM) services, at least in one district, are available in 14 States, except Jharkhand and Gujarat. (UNICEF Continuity of Services Tracking, September 2021)
- Nutrition Rehabilitation Centers (NRCs) providing inpatient management of severe acute malnutrition have returned to normal operational in most States/UTs. (UNICEF Continuity of Services Tracking, September 2021)
- Active screening for acute malnutrition among children under five years was conducted during September 2021 in Telangana, Uttar Pradesh, West Bengal, Rajasthan, Maharashtra (more than more than 18,500 children were identified with SAM and have been enrolled for appropriate care and management under VCDC or NRC), Madhya Pradesh, Karnataka, Gujarat and Assam. (UNICEF Continuity of Services Tracking, September 2021)
- Under the Home Based Young Child (HBYC) programme, ASHAs and ANMs are visiting households and promoting IYCF practices regularly. (UNICEF Continuity of Services Tracking, September 2021)

Anganwadi worker Vidhya Jain (Left) weighs a child at the Jethana B Anganwadi center, Rajasthan, 24 Dec 2020. Photo © Sri Kolari
5.2. School age children and adolescents
- Schools remain closed and most of the States/UTs have not taken any decision regarding reopening of the elementary classes which are the target groups for the MDM. The MDM is reported to be functional in in one form or another in 35 of 36 States/UTs (except in ) Nineteen States/UTs are providing dry rations and other food items, whereas 16 others are providing dry rations with cooking cost as Food Security Allowance, up to the period of summer vacation. The food items provided include mostly grains complemented with pulses, oil, potatoes, eggs plus salt and condiments, which vary from place to place. (WFP MDM Tracking, April to June 2021)
- The SCHOOL survey conducted among 1400 school children in underprivileged households in August 2021 found MDMs were discontinued in all the sampled States with schools Among parents with a child enrolled in a government school, 80% reported receiving some food (mainly rice or wheat) during the preceding 3 months as substitute for midday meals, a small minority received any cash, and a significant proportion did not receive anything during that period. Among those who received food, there were complaints that the parents had received less than what they were entitled to (100 grams per child per day at the primary level). Most parents wanted reopened schools as soon as possible.
- There is reduction on IFA supplementation among children aged 5-9 years (March 2020 versus June 2021 is 18.9% versus 8.9%) as well as among school children attending 6-12 class (March 2020 versus June 2021 is 23.2% versus 16.5 %.) (HMIS)
- Similarly, there is also reduction on deworming among children aged 5-9 years (March 2020 versus June 2021 is 2.9% versus 0.5%) as well as among school children attending 6-12 class (March 2020 versus June 2021 is 3.2% versus 0.5%. (HMIS)
- There is reduction on IFA supplementation among out of school adolescent girls 10-19 years at AWCs: March 2020 versus June 2021 is 14.7% versus 8.3%. (HMIS)
- Similarly, there is also reduction on deworming among out of school adolescent girls 10-19 years at AWCs: March 2020 versus June 2021 is 1.7% versus 0.3%. (HMIS)
- There is no information on the Health / Nutrition assessments among adolescents.
5.3. Women of Reproductive Age
- The IFA supplementation among pregnant women reported for March 2020 versus June 2021 is 9% versus 89.7%. (HMIS)
- Deworming among pregnant women after first trimester reported for March 2020 versus June 2021 is 47.1% versus 49.2%. (HMIS)
- The IFA supplementation among lactating women reported for March 2020 versus March 2021 (data unavailable for subsequent months) is 49.2% vs. 53.7%. (HMIS)
- Calcium supplementation among pregnant women reported for March 2020 versus February 2021 (proportion unavailable for subsequent months) is 73.2% versus 81.7%. (HMIS)
- There is reduction in pregnant women receiving four or more ANC check-ups as reported for March 2020 versus June 2021 is 73.1% versus 62.6%. (HMIS)
- Similarly, there is also reduction in institutional deliveries as reported for March 2020 versus June 2021 is 62.1% versus 48%. (HMIS)
- The THR for pregnant and lactating women are reported to be functional in all states. (UNICEF Continuity of Services Tracking, September 2021) In Jharkhand and Rajasthan, sharing of the THR for pregnant and lactating women with other family members was reported during August 2020 increasing the risk of dilution of the intended nutritional benefits (IDinsight May 2021)
- The PMVVY (maternity benefits) is reported operational in all states (UNICEF Continuity of Services Tracking, September 2021)
5.4. Nutrition Social Behaviour Change Communication Activities
- Village Health Sanitation and Nutrition Days (VHSNDs) are functional in all 14 States/UTS. (UNICEF Continuity of Services Tracking, September 2021)
- Poshan Pakhwada, 16-31 March 2021, was celebrated across the country. Total 22,148,308 activities were conducted and total 969,343,702 beneficiaries were reached. (Jan Andolan database)
- World Breastfeeding Week, 1-7 August 2021: The Ministry of Health and Family Welfare (MoHFW) strongly promoted exclusive and continued breastfeeding through statements and highlighted previously released guidance emphasising the importance of breastfeeding amidst COVID-19.
- Poshan Maah, September 2021 was celebrated at national and sub-national levels across the The data on number of activities conducted and target groups reached with the behaviour change events are yet to become available at the Jan Andolan database.
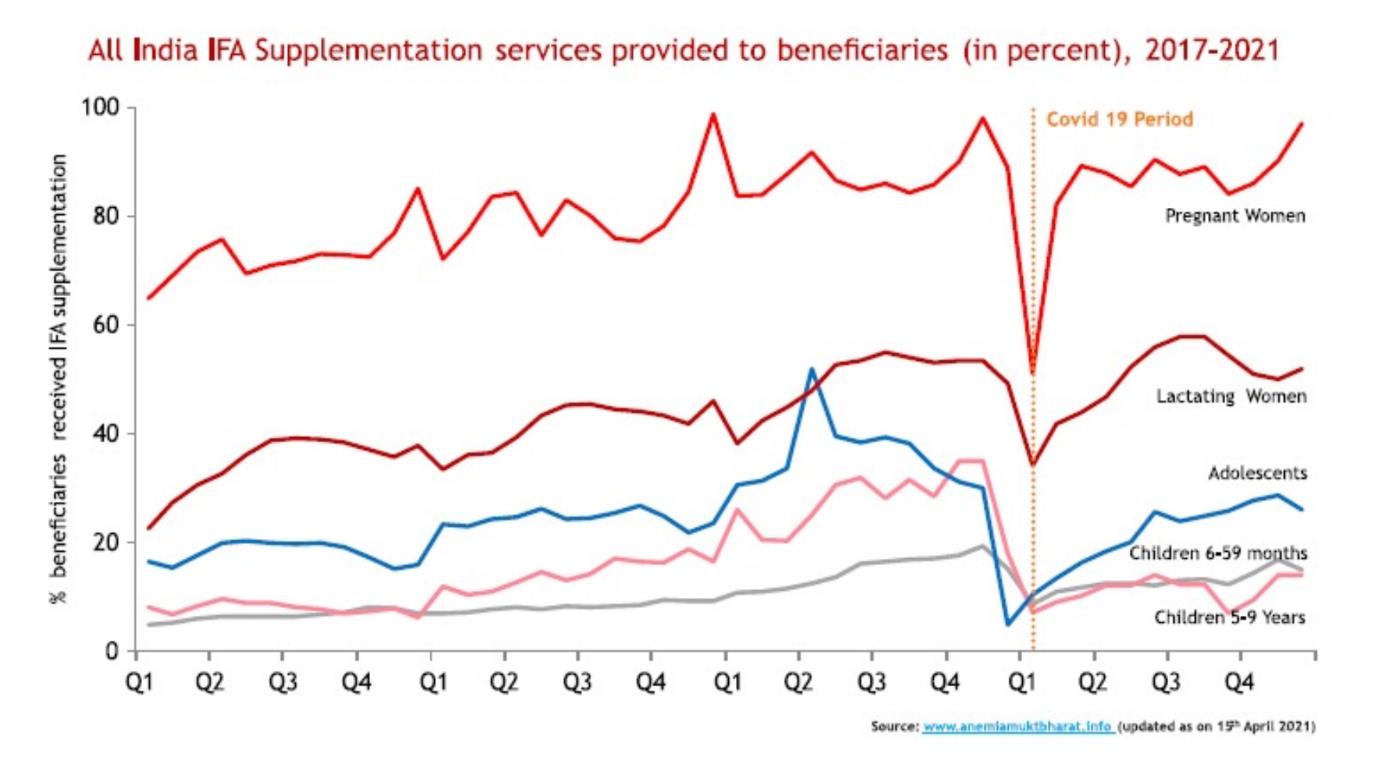
Source: AnemiaMuktBharat.info
5.5. Fortification
- The Government of India committed to provided Iron Fortified Rice through the Public Distribution System, Mid Day Meals and Take Home Rations from the AWCs by
- Industry partners increased their capacity for production of fortified of edible oil (~ 299 oil producers across 14 States, currently fortifying 8.1 million metric tonnes (MT) per year with potential to reach 901 million beneficiaries), milk (~107 milk dairies across 12 States/UTs to fortify 4.8 million liters of fortified milk per day reaching 24 million beneficiaries), and wheat flour (~84 wheat flour mills across 3 States to fortify 0.4 million MT of wheat flour per year reaching 27 million beneficiaries under the social safety net programmes, additionally 24,005 MT of fortified wheat flour is produced per year reaching 0.3 million people through the open commercial market (GAIN, September 2021).
6. Nutrition Sensitive Sector Updates
6.1 Food Security
- A rapid assessment conducted on the effect of COVID-19 induced lockdown among 5,162 rural households across 12 States and 47 districts during May 2020 had documented negative coping mechanisms such as reduction in food item in meals, reduction in number of meals, borrowing of food grains, taking loans, selling of assets and mortgage of household items. There was also large dependence on the TPDS. Similar findings were also documented in a joint rapid assessment conducted in Odisha during June 2020 (IAG and WFP, June 2020.)
- A household survey conducted via phone in districts of Uttar Pradesh found that Household Food Insecurity increased sharply from 21% in December 2019 to 80% in August 2020, with 62% households changing the status from food secure to insecure over this period. Children in newly or consistently food-insecure households were less likely to consume a diverse diet compared with those in food-secure households. (IFPRI and Alive & Thrive 2021)
- The TPDS reported to provide much needed relief to the vulnerable families across the country. Expanded rations/pulses were distributed under third phase of Pradhan Mantri Garib Kalyan Anna Yojana reaching 94% coverage in May 2021. The ration distribution found to help the beneficiaries during the crisis (Dalberg, May 2021 ) but the need to improve inclusion of eligible beneficiaries also highlighted.
- Food prices varied greatly at the beginning of the lockdown in April 2020. Nutritious food like eggs increased in cost between February and April 2021. (GAIN, June 2021)
- Food insecurity highlighted as a serious concern in numerous assessments from across the country, more so among the disadvantaged groups, during and after the national lockdown period of late March to end of May 2020 (Dreze & Somanchi, May 2021)
6.2. Health
- Immunization and health check-ups are functional through home visits or at the AWCs despite the reported AWCs closures. (WFP ICDS Tracking, January to April 2021)
- HMIS data show significant increase in maternal mortality in May 2021 mainly from other/unknown causes – over 82% increase over maternal deaths reported in May 2019.
- There was significant decrease in hospital births per month and increase in overall case fatality of complications by 23% in data from 15 hospitals from 5 states during the pandemic (Nair et al. 2021)
- During April to December 2020, child immunizations was reported low across 16 States and particularly among Muslims and urban poor. (COLLECT Dashboard)

12
6.2. Health
• Immunization and health check-ups are functional through home visits or at the AWCs despite the reported AWCs closures. (WFP ICDS Tracking, January to April 2021)
• HMIS data show significant increase in maternal mortality in May 2021 mainly from other/unknown causes – over 82% increase over maternal deaths reported in May 2019.
• There was significant decrease in hospital births per month and increase in overall case fatality of complications by 23% during the pandemic period. (Nair et al. 2021)
• During April to December 2020, child immunizations was reported low across 16 States and particularly among Muslims and urban poor. (COLLECT Dashboard)
Rehana Pathan (ANM) immunize a child at the Jethana Sub Health Center, Rajasthan, 24 Dec 2020. Photo © Sri Kolari
6.3. WASH
- Efforts to promote WASH at state level: activities such as promotion of hand washing, safe drinking water and open defecation free status are being conducted in Odisha, Jharkhand, Uttar Pradesh and Gujarat. (Rapid Survey Findings, WeCAN)

Anganwadi worker Leena Bhat (Left) demonstrating the best ways to wash hands with soap.
Jethana, Rajasthan, 24 Dec 2020. Photo © Sri Kolari
6.4 Early Childhood Development (ECD)
- Efforts to revive ECD activities are being made. Seventeen States/UTs are focusing on pre-school education component using digital and/or mass media platforms (WFP ICDS Tracking, January to April 2021.)
- Preparations to start ECD activities are being made in Maharashtra and (UNICEF Continuity of Services Tracking, August and September 2021)
6.5. Governance
- Calls for sufficient budgetary allocations for nutrition related trainings and essential supplies for distribution by frontline workers as well as the need to address gaps in supply chains (CRY and CBGA 2021)
- Attention has been drawn for increased government funding and resources in the recent years for improvements in the levels of child nutrition, anaemia and
6.6. Gender and Equity
- Gender inequality and inequity in workload, job losses and recovery: increase in unpaid responsibilities for women – 47% of women (compared to 43% of men) reported an increase in chores and 41% of women (compared to 37% of men) reported an increase in unpaid care work; 32% rural men lost paid work during the peak of the crisis (compared to 41% of rural women) and only 4% are yet to recover compared to 11% of rural women; more women from historically marginalized groups affected including women from lower-income households, Muslim, migrant women, and single separated/divorced women. (Dalberg May 2021 report)
- Increased vulnerability to hunger and malnutrition reported in tribal communities of Jharkhand due to COVID-19 pandemic.
- The rapid assessment conducted on the effect of COVID-19 induced lockdown among 5,162 rural households across 12 States and 47 districts during May 2020 had documented increase in workload among women.

Ankush Nanoma and his wife Rekha Nanoma old play with their two children at home, Jethana village, Rajasthan, 24 Dec 2020. Photo © Sri Kolari
6.7. Livelihoods
- Disruptive impact of COVID-19 pandemic on livelihoods, especially among the poor and vulnerable, along with a significant rise in MGNREGA employment scheme: according to Ministry of Rural Development, more than 18 million were offered work in May 2021, a 52 per cent rise from figures recorded during the same period in May 2019. The scheme reported as particularly beneficial for women from low-income households.
- During April to December 2020, 40% hamlets in vulnerable communities/excluded groups across 16 States reported not having any job under MNREGA and an increase in indebtedness, especially in urban areas (COLLECT Dashboard.)
- The rapid assessment conducted on the effect of COVID-19 induced lockdown among 5,162 rural households across 12 States and 47 districts during May 2020 had documented reduced income from key livelihood activities.
7. Key Global Updates
- The Impact of COVID-19 pandemic on Food Security and Nutrition: Disruption in food security and nutrition due to COVID-19 pandemic can result in consequences for health and nutrition of a severity and scale unseen for more than half a century (UN June 2020). Given the massive impact on food and nutrition security, there have been calls for strategic action to build resilient food systems amidst the pandemic (Suri, Aug 2021.)
- The newborn survival benefit of close contact from Kangaroo Mother Care far outweighs the small risk of death due to COVID-19, especially in the low and middle income countries (Minckas et al. Feb 2021.)
- A longitudinal study from Rhode Island, USA found that children born during the pandemic score markedly lower on standard measures of verbal, motor, and overall cognitive ability (Dyer, Aug 2021.)
- Due to significant disruptions in nutrition and lifestyle habits of children, undernutrition is expected to worsen in poor countries and obesity rates could increase in middle- and high-income countries especially among precarious groups widening the gap in health and social inequalities (Zemrani et al., Jan 2021.)
8. Stories highlighting Poshan-COVID specific initiatives/innovations
8.1 An attempt at reaching the last mile during COVID-19 – Virtual tracking of severely malnourished children (TATA Trusts)
The unprecedented nationwide shutdown initially planned for 21days, extended multiple times to counter the surge of increasing cases. A direct consequence of which was slowing down of almost all other activities including shutdown of physical Anganwadi Centres, while services continued. With multiple extension of lockdowns, it became imperative to find other ways to reach out to already on the verge kids and mothers in tribal areas. Finding roots in resuming activities virtually, it’s a story of finding and treating a SAM child.
Before Intervention
Most children due to disruption in growth monitoring services due to Anganwadi closure have gone unnoticed or unidentified. Children who were moderately undernourished and need extra services from ICDS by way of availing additional supplemental nutrition for weight and appropriate counselling, have been tipping into severe cases in the absence of timely assessment. Rajib (name changed), a 4 year old in Sonale village of Palghar, was a SAM child and went unnoticed due to hampered services. Govt. of Maharashtra under its ICDS scheme supplies Energy Dense Nutritious Food (EDNF) to children suffering from severe wasting. However, for beneficiaries to avail of those services, one, beneficiaries themselves need to be aware of the condition of the child or aware of the services provide. Two, frontline workers need to actively identify cases of severe wasting through monthly scheduled growth monitoring sessions and make weight appropriate EDNF available to the child. When either of it fails, the system collapses.
Trusts Intervention
Nevertheless to say, pandemic has been testing times and each one is trying their best to reach out to the most vulnerable. Reaching out to the beneficiaries at first appeared to be a herculean task, however, leveraging technology by forming Whatsapp groups with frontline workers paved way. Trusts field coordinators through audio/video calls with Anganwadi workers, could access beneficiary contact details from their registers or CAS mobile. Frontline workers were trained and counselled to resume reaching out to children virtually and resume the conduct of Village Health and Sanitation Days with appropriate precautions. While reaching out to mothers and children of the village, Rajib was found, who was sick in the past few days. Anganwadi worker through the previous trainings on convergence, along with ASHA and ANM reached out to Rajib’s parents. Upon taking his anthropometric measurements, he was found to be severely wasted but did not show any signs of complications. He was registered for availing EDNF as well as additional supplementary nutrition under ICDS. His parents were counselled and hand held on modifying his diet appropriately using local ingredients as well as Take Home Ration. They were also made aware of the services they can avail and the importance of growth measurement.
After Intervention
A month later, Rajib started recovering and gained weight as well as height. He was now categorized as moderately wasted. A close contact with Anganwadi worker and his parents helped the child in need as he is on his path to recovery. His parents are continuously hand held by Trusts field coordinators through the use of video calling and he is under close watch of Anganwadi worker, ANM, ASHA as well as Sarpanch through the convergence matrix adopted to ensure he becomes normal soon.
8.2 Human Milk Bank Testimonials (PATH)
“The establishment of a CLMC at the King George Medical University Hospital has been a boon to ensure optimal feeding for our vulnerable infants. PATH’s support towards the establishment and running of this initiative in general, especially during COVID times has been very valuable. Owing to the novel nature of the pandemic, our health care workers and mothers had concerns and questions on how to safely feed the newborns. PATH’s support in the form of evidence-based guidance for health care providers and resource materials for mothers have helped in dispelling doubts and addressing concerns.”~ Dr. Mala Kumar Professor, Paediatrics, King George Medical University, Lucknow
“I am thankful to PATH for helping us establish the state’s first CLMC at Jay Prakash Hospital in Bhopal, Madhya Pradesh. This centre has been instrumental in providing exclusive human milk to newborns, even during COVID-19. During the lockdown period, we had several questions about the smooth operations at the CLMC. PATH provided us timely assistance, mentoring support, and communications resources based on the latest global and national guidance and helped resolve our concerns. With our joint efforts, the CLMC has been able to provide uninterrupted maternal and newborn nutrition and care services to mothers and babies.” ~ Dr. Asha Dixit Paediatrician and In-Charge CMLC, JP Hospital, Bhopal
9. Abbreviations
ANM Auxiliary Nurse Midwife
ASHA Accredited Social Health Activist
AWC Anganwadi Centers
BMI Body Mass Index
CMAM Community-based Management of Acute Malnutrition
CNNS Comprehensive National Nutrition Survey
IFA Iron Folic Acid
HMIS Health Management Information System
POSHAN Prime Minister’s Overarching Scheme for Holistic Nutrition MNREGA Mahatma Gandhi National Rural Employment Guarantee Act MOHFW Ministry of Health and Family Welfare
MOWCD Ministry of Women and Children Development
NFHS National Family Health Survey
MDM Mid-day Meal
PMGKAY Pradhan Mantri Garib Kalyan Anna Yojana
PMMVY Pradhan Mantri Matru Vandana Yojana
SAM Severe Acute Malnutrition
TPDS Targeted Public Distribution System
UNICEF United Nations Children’s Fund
UT Union Territory
WASH Water Sanitation and Hygiene
WFP World Food Programme
To contribute or request further information please contact: <poshan@unicef.org>
To download the PDF version of the report click here